


NASHVILLE, TENNESSE
In April of 2005, I was in my last semester of college at Lipscomb University when I lost the vision in my left eye. I had just gotten back from Spring Break in Cancun with my mom, Katie & Patti when the unheard of happened.
I lived alone at the time, and as I was getting ready for school one morning, while putting on my eye liner, I realized that I could no longer see myself when I closed my right eye. This was very upsetting as I'd had vision corrective surgery in February of 2002 ... so for my eyes to be anything other than 20/15, something was obviously wrong.
My grandmother took me to see my eye doctor, and you know something isn't good when your doctor unnervingly gasps. He felt it was either a tumor or Choroidial Neo-Vascularization (CNV). He sent me to a retina specialist who diagnosed me with CNV and said the root of the problem was idiopathic. I then went through 3 laser surguries called photocoagulation with an additional round of steriods. As of April 2007, I was pronounced stable with no office visits for a year, and only a 5% chance of getting the same disease in my right eye.
GRAND RAPIDS, MICHIGAN
On July 21, 2007, Steve and I were married and moved to Grand Rapids, Michigan on August 4th. Having to re-establish myself with new doctors, I quickly made an appointment at Grand Rapids Ophthalmology. It wasn't long before I had an appointment with Dr. Yosef Gindzen, one of the top retina specialists in the country. On my first office visit, he asked me if I grew up near the Mississippi River. It was that day I learned about Ocular Histoplasmosis.
*** Fact ****
In the United States, the highest incidence of histoplasmosis occurs in a region often referred to as the "Histo Belt," where up to 90% of the adult population has been infected by histoplasmosis. This region includes all of Arkansas, Kentucky, Missouri, Tennessee, and West Virginia as well as large portions of Alabama, Illinois, Indiana, Iowa, Kansas, Louisiana, Maryland, Mississippi, Nebraska, Ohio, Oklahoma, Texas, and Virginia. Since most cases of histoplasmosis are undiagnosed, anyone who has ever lived in an area known to have a high rate of histoplasmosis should consider having their eyes examined for histo spots.
**********************
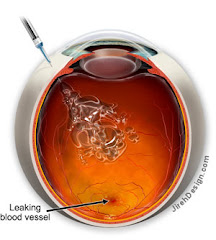
Dr. Gindzen noticed histospots (CNV) in my right eye located right at my central vision. Though they were smaller and fewer in number than those in my left eye, they were there nonetheless, sending that 5% chance of activity to nearly 100% ... vision loss inevitable and dependent only on when the little terriorists woke up and decided to grow. Now, my left eye, which was pronounced "stable" less than a year ago, already had new growth activity and blood leakage, but we've decided not to treat it at the moment since there is already no central vision. Once it begins to expand into what peripheral vision I have left, we'll begin Avastin injections.
Every morning I look at my Amsler Grid to note any changes in vision. Three weeks ago, my right eye grid became distorted. A growth had woken up and was making itself known. Yesterday, March 10, 2008, I began Avastin injections for the first time in my right eye. Waiting those three weeks has thrown my overall vision off enough to cause daily headaches and night driving to be even more difficult, but I have faith I'll adjust to that change soon. There is a 40% chance that the Avastin injections will work and the distortion in my only good eye will be restored to normal.
Unlike photocoagulation treatments which left me with scarred tissue causing permanent blindness at my macula (central vision), Avastin injections leave no scarring, except that one could need them as often as every 4-6 weeks ... sometimes indefinitely. I've spoken to some people who've been getting these intravitreal injections for years. I can't even imagine going through that but I've started the journey now, so pretty soon, I will be one of them ... A Histo Groupie.
I have added some information below about Ocular Histoplasmosis Syndrome. This is not a widely known disease and most people who are carriers have no idea the kind of monster that lies in their system. Thankfully, most people's immune systems are strong enough to kick this nasty disease ... only experiencing symptoms of a common cold or flu. But those who are physically and emotionally impacted by OHS struggle with it for a lifetime as it never fully goes away.
Thank you for reading my story and I hope, in some way, I was able to provide some information about OHS through my personal experience and the collection of data below. On behalf of myself and other OHS victims, please keep us all in your prayers as we struggle daily with our present vision lost as well as knowing that a near end is not in sight.
1 comment:
You are in my prayers chicka! love ya! Amy
Post a Comment